
 English
English
Last updated on April 9th, 2022
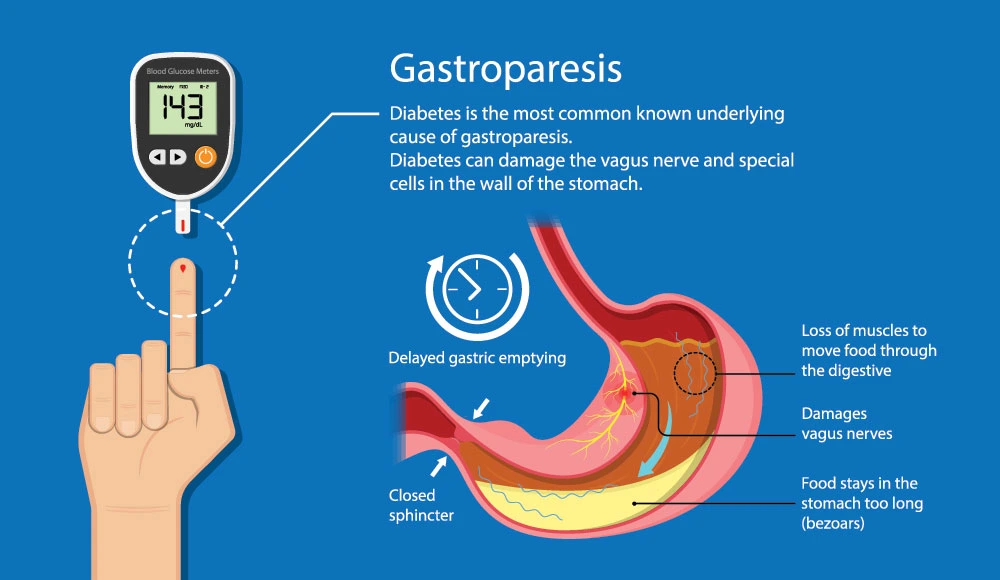
Diabetic gastroparesis is a complication of poorly controlled diabetes mellitus, resulting from dysfunctions of the autonomic and enteric nervous systems. These conditions cause a delay in gastric emptying.
They may develop the presence of upper gastrointestinal symptoms, especially: early satiety, vomiting, nausea, anorexia, and weight loss, in addition to abdominal distension and pain. It is noteworthy that some patients have diabetes and intestinal problems symptoms associated with regular gastric emptying, while others have mild or absent symptoms even if there is abnormal gastric emptying.

What are the Symptoms of Diabetic Gastroparesis?
Here is the list of diabetic gastroparesis symptoms a person might feel:
- Acidity
- Nausea
- Threw up
- lack of appetite
- inflammation
- poor glycemic management
Untreated diabetic gastroparesis will result in food remaining in the stomach for a long time, developing bacteria and other stomach obstructions.

What is the Relationship Between Gastroparesis and Diabetes?
Summary
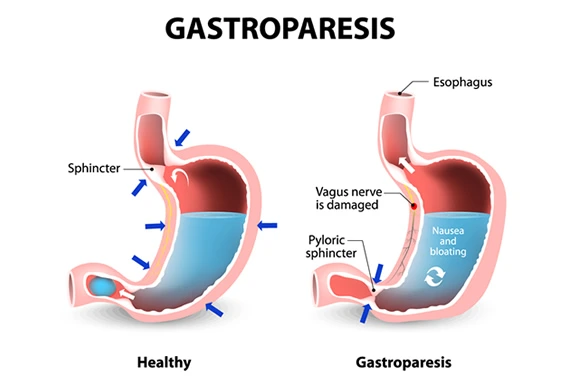
Gastroparesis can transpire in both type 1 and type 2 diabetes. Gastroparesis can damage the vagus nerve, which controls the stomach muscles. It is believed that the combination of high blood glucose and insulin deficiency can cause this vagus nerve damage.
Etiology
This pathology affects 20% to 50% of diabetic patients, especially those diagnosed with type 1 diabetes mellitus or those diagnosed with type 2 diabetes gastroparesis for more than ten years. In these cases, delayed gastric emptying can occur in up to 65% of patients with type 1 DM compared to 30% of patients with type 2 DM. Regarding prevalence, proportionality is observed according to increasing age. Furthermore, most studies demonstrate a higher prevalence in women than in men.
Pathophysiology
The pathophysiology of diabetic gastroparesis infers that hyperglycemia or inefficient glucose uptake favors neuronal damage that promotes abnormality in myenteric neurotransmission, impairment of inhibitory neuronal function, and dysfunction in smooth cells and interstitial cells of Cajal. These dysfunctional sets cause less antral contraction, a disorder in antro-duodenal contractions, in addition to pylorus spasms, consequently favoring delayed gastric emptying. Therefore, this slowdown in emptying causes more excellent carbohydrate absorption, selecting higher glucose levels.
What is the Impact of Diabetic Gastroparesis on Quality of Life?
Quality of life is significantly impaired, especially in patients with abdominal pain, nausea, and vomiting. Thus, many patients develop mood disorders, of which 50% and 38% report anxiety and depression, respectively. About 66% of patients who present abdominal pain as a symptom have sleep interference since this pain is usually epigastric, postprandial, and nocturnal.
How to Diagnose Diabetic Gastroparesis?
Summary
According to the American College of Gastroenterology, the combination of upper gastrointestinal signs and symptoms associated with delayed gastric emptying, excluding ulcerations or gastric outflow obstruction, is necessary to diagnose this pathology. However, in addition to clinical history and physical examination, other diagnostic techniques can be used.
Gastric Scintigraphy
The low-cost, gold standard test is gastric scintigraphy, as it provides a physiological, non-invasive, and quantitative measure for evaluating gastric emptying of a radiolabelled solid meal. Indications for this test are diabetic patients with upper gastrointestinal symptoms, poor glycemic control, those being treated with hypoglycemic medications that can delay gastric emptying, and patients with severe reflux symptoms that do not respond to standard therapy. Gastric scintigraphy should be performed after excluding mechanical or structural causes of abnormal gastric emptying.
Also Read: Normal Blood Glucose Levels
Upper Digestive Endoscopy (EDA)
Upper digestive endoscopy (OTE) is essential to rule out strictures, ulcers, or masses.
Breath Test for Stable Gastric Emptying
It is a test performed using a stable isotope – C-octanoic acid – and has been a promising alternative to scintigraphy. It is a non-invasive diagnostic method, and, unlike scintigraphy, it does not expose the patient to radiation and can be used in pregnant women, nursing women, and children. However, in general, it is indicated for cases in which scintigraphy is not feasible.
Electrogastrography
This test can be helpful as an additional diagnostic test for diabetic gastropathy diagnosis. It works by measuring slow-wave gastric myoelectric activity, usually from skin electrodes placed along the long axis of the stomach, performing a preprandial recording for about 45 to 60 minutes. After this period, the patient receives a meal, followed by a 45-60 minute postprandial recording. Although this test is potentially helpful, it is not yet available for general clinical use.
Ultrasound
By analyzing transverse changes in the volume remaining in the stomach antrum over time, ultrasonography can be used to evaluate the emptying of a liquid meal. In addition, three-dimensional ultrasonography has recently been developed and reported to help determine gastric function, and duplex ultrasonography quantifies the transpyloric flow of liquid gastric contents. It is noteworthy that these techniques are preferable to scintigraphy in pregnant women and children to minimize radiation exposure.
Also Read: Diabetes and Thyroid Disorders
What is the Proper Treatment For Diabetic Gastroparesis?
Treatment’s primary goal is to improve quality of life, ensure sufficient nutritional intake, control the progression, reduce symptoms and signs of diabetic gastroparesis. The use of lifestyle changes and medications are essential: adequate glycemic control and cessation of smoking and alcoholism.
Nutritional Management
Nutritional management must be carried out effectively from a balanced diet through smaller and more frequent meals during the day and with reduced-fat and fiber content (they tend to delay gastric emptying). It encourages the intake of fluids during meals and, after eating, it is recommended that the patient remain seated for 1 or 2 hours.
Also Read: Can Type 2 Diabetes be Cured Permanently?
Pharmacological Management of Diabetic Gastroparesis
Antiemetic Drug
They are essential because they help control symptoms such as vomiting and nausea. The most commonly used medications are serotonin receptor antagonists (ondansetron) and dopamine receptor antagonists (promethazine). It is noteworthy that the side effects of these medications include sedation and extrapyramidal effects.
Prokinetic Agents
The metoclopramide – receptor activating 5-HT4 receptor antagonist and dopamine receptor in the stomach with low antagonism of 5-HT 3 receptors in the nervous system – is a common drug used in diabetic gastroparesis and diabetic stomach treatment, it therefore, promotes increased contraction amplitude esophageal musculature and gastric – fundic and antral.
The Domperidone is a dopamine antagonist metoclopramide and resembles, although with fewer side effects to the central nervous system. It has been shown to reduce gastrointestinal symptoms and hospitalizations for gastroparesis and accelerate gastric emptying. Furthermore, it can cause gynecomastia in men and amenorrhea and galactorrhea in women. It is essential to perform an electrocardiographic evaluation as this medication can cause cardiac arrhythmias.
Erythromycin is a macrolide antibiotic with an agonistic effect on motilin receptors in the gastrointestinal tract, thus increasing gastric emptying. However, the QT interval can be prolonged with its use. Therefore, electrocardiographic evaluation is essential before and during treatment.
Also Read: Health Benefits of Saunf Seeds
Endoscopic and Surgical Treatment
Ventilating gastrostomy is a procedure based on the placement of a ventilation tube endoscopically, usually postprandially, about six or five times a week in patients with idiopathic gastroparesis. Although there is no evaluative study on the effect of this procedure in patients with diabetic gastroparesis, the diabetic gastroparesis treatment guidelines set by the American College of Gastroenterology state that, in some conditions, ventilation gastrostomy can be performed in these patients.
In general, enteral nutrition is preferable to parenteral nutrition in patients who cannot tolerate the oral diet so that enteral nutrition can be provided through a jejunostomy. The procedure is performed using direct percutaneous jejunostomy, often associated with ventilation gastrostomy.
In addition, other procedures are endoscopic pyloroplasty and transpyloric stent placement, which have shown substantial improvement in symptoms and gastric emptying. This last method has been proposed as rescue therapy and as a bridge to permanent treatments such as gastric electrical stimulation.
Gastric electrical stimulation can be performed by implanting electrodes along the greater curvature of the stomach. This therapy can be used mainly to treat nausea and vomiting secondary to gastroparesis.

Conclusion
From the above, the need for future research in epidemiology, pathophysiology, and, mainly, in the treatment of diabetic gastroenteropathy becomes evident. Most studies on the pathology are relatively small. Currently, it is observed that treatment depends, above all, on gradual approaches that incorporate dietary modifications, glycemic control, and the use of antiemetic and prokinetic medications. However, there are some more invasive therapeutic procedures understudy and analysis.
In general, knowledge about diabetic gastroparesis is still reserved. Endoscopic and surgical therapies have promising futures, but there are still few studies and clinical trials that more adequately prove their effectiveness. Therefore, research aimed primarily at understanding the pathophysiology and treatment of diabetic gastroparesis symptoms should be encouraged to more adequately validate the therapeutic procedures’ tolerability, advantages, and disadvantages.
Also Read: Early Symptoms of Diabetes
FAQs:
When did you need to call your healthcare provider?
It is important to keep a track of your health conditions during diabetes. Connect with your healthcare provider if you witness any of these symptoms, such severe abdominal pain, unable to retain food or liquids down, unexplained weight loss, inability to control blood sugar (too high or too low) and other symptoms that are indicated by your healthcare provider.
What are the complications with diabetic gastroparesis?
Food can ferment in the stomach. This causes the growth of bacteria. Undigested food can also harden into a mass called a bezoar. This can lead to nausea and vomiting. In some cases, they can prevent food from passing from the stomach to the small intestine. Gastroparesis can make it challenging to manage blood sugar levels. It can also cause problems for the body to absorb vitamins and minerals.
How does diabetes affect the digestive system?
Poor control of type -2 diabetes can lead to various digestive disorders. Basically, increasing blood sugar levels leads to neuropathy, which in turn increases the risk of health issues such as acid reflux and gastroparesis. Common digestion issues should never be ignored in case of diabetic patients.
Is gastroparesis dangerous?
Although diabetes gastroparesis is not so dangerous, but it definitely can cause serious complications if not treated on time. Some of the complications it can cause include malnutrition, dehydration, and can lead to a situation where it blocks the flow of food out of stomach.
What are the causes of diabetic gastroparesis?
The specific vagus nerve helps control the movement of food throughout the digestive system. This nerve can be damaged due to chronic high blood sugar caused by diabetes that is not well treated. This causes food to move slowly or to stop moving. They push food to digest.
References:
Last Updated on by Dr. Damanjit Duggal
Disclaimer
This site provides educational content; however, it is not a substitute for professional medical guidance. Readers should consult their healthcare professional for personalised guidance. We work hard to provide accurate and helpful information. Your well-being is important to us, and we value your feedback. To learn more, visit our editorial policy page for details on our content guidelines and the content creation process.








{kind=link}